Liver and Gallbladder
The falciform ligament (with the ligamentum teres at its free margin) is the embryonic remnant of the ductus venosus (umbilical vein) of the umbilical cord. It is a peritoneal structure that courses between the anatomical left and right lobes of the liver and the anterior abdominal wall.
As the falciform ligament passes onto the superior surface of the liver, the two layers of peritoneum diverge to the right and to the left, creating the anterior layers of the coronary ligaments.
These pass to the right and to the left to the extremes of the superior liver surface, turn back on themselves (creating the triangular ligaments), and turn posteriorly to form the posterior layers of the coronary ligaments. In this manner, an area devoid of visceral peritoneum is created, the bare area of the liver.
The posterior layers of the coronary ligaments converge to form the lesser omentum, which passes from the visceral surface of the liver to the lesser curvature of the stomach (hepatogastric ligament) and the first part of the duodenum (hepatoduodenal ligament).
The liver is divided anatomically into four lobes by external landmarks and is delineated on the visceral surface by fissures and fossae, which form the letter H.
The right side of the H is formed by fossae for the gallbladder and the IVC, and the right lobe lies to the right of these structures. The left side of the H is formed by the fissure for the round ligament and the ligamentum venosum (adult remnant of the ductus venosus); the left lobe is to the left of this fissure. The crossbar of the H is the porta hepatis, through which the hepatic artery, portal vein, and nerves enter the liver and the bile ducts and lymphatics exit.

The visceral surface of the liver. (from Lindner HH. Clinical Anatomy. East Norwalk, CT: Appleton & Lange, 1989:399.)
The crossbar subdivides the central portion into quadrate and caudate lobes. Functionally, the right portal lobe lies to the right of the fossae of the gallbladder, IVC, and a portion of the caudate lobe. The left portal lobe is the left anatomical lobe, quadrate lobe, and the remainder of the caudate lobe. The portal lobes are supplied by lobar branches of the hepatic artery, portal vein, and bile ducts. Although lacking external landmarks, the portal lobes are further divided functionally into hepatic segments.
The larger right lobe occupies the right hypochondrium has two additional smaller lobes at its posterior-inferior surface, the caudate and quadrate lobes.
The smaller left lobe is flatter and is situated in the epigastrium and left hypochondrium.
Surgical Anatomy
In contrast, surgical anatomy divides the liver based on its blood supply. Thus, the right and left surgical lobes are defined by the point of bifurcation of the hepatic artery and portal vein (porta hepatis); the falciform ligament therefore divides the left surgical lobe into medial and lateral segments. Surgical anatomy defines a total of eight segments.
{
-
The left anatomical lobe, quadrate lobe, and a portion of the caudate lobe constitute the left portal lobe.
-
The portal vein drains blood from organs supplied by the celiac artery, superior mesenteric artery (SMA), and inferior mesenteric artery (IMA).
-
As the falciform ligament passes onto the superior surface of the liver, the two layers of peritoneum diverge to the right and to the left, creating the anterior layers of the coronary ligaments. These pass to the right and to the left to the extremes of the superior liver surface, turn back on themselves (creating the triangular ligaments), and turn posteriorly to form the posterior layers of the coronary ligaments. In this manner, an area devoid of visceral peritoneum is created, the bare area of the liver. The posterior layers of the coronary ligaments converge to form the lesser omentum, which passes from the visceral surface of the liver to the lesser curvature of the stomach (hepatogastric ligament) and the first part of the duodenum (hepatoduodenal ligament).
The liver is covered with visceral peritoneum over most of its surface and is suspended by several mesenteric structures called ligaments.
The falciform ligament (with the round ligament of the liver, the adult remnant of the umbilical vein, in its free margin) is reflected onto the anterior abdominal wall and divides the liver into apparent right and left anatomical lobes.
As the falciform ligament passes onto the superior surface of the liver, the two layers of peritoneum diverge to the right and to the left, creating the anterior layers of the coronary ligaments.
These pass to the right and to the left to the extremes of the superior liver surface, turn back on themselves (creating the triangular ligaments), and turn posteriorly to form the posterior layers of the coronary ligaments.
In this manner, an area devoid of visceral peritoneum is created, the bare area of the liver. The posterior layers of the coronary ligaments converge to form the lesser omentum, which passes from the visceral surface of the liver to the lesser curvature of the stomach (hepatogastric ligament) and the first part of the duodenum (hepatoduodenal ligament).
The liver is divided anatomically into four lobes by external landmarks and is delineated on the visceral surface by fissures and fossae, which form an “H.” (See Figure Below).
The visceral surface of the liver. (Reproduced, with permission, from Lindner HH. Clinical Anatomy. East Norwalk, CT: Appleton & Lange, 1989:399.)
The right side of the H is formed by fossae for the gallbladder and the IVC, and the right lobe lies to the right of these structures. The left side of the H is formed by the fissure for the round ligament and the ligamentum venosum (adult remnant of the ductus venosus); the left lobe is to the left of this fissure. The crossbar of the H is the porta hepatis through which the hepatic artery, portal vein, and nerves enter the liver and the bile ducts and lymphatics exit. The crossbar subdivides the central portion into quadrate and caudate lobes. Functionally, the right portal lobe lies to the right of the fossae of the gallbladder, IVC, and a portion of the caudate lobe. The left portal lobe is the left anatomical lobe, quadrate lobe, and the remainder of the caudate lobe. The portal lobes are supplied by lobar branches of the hepatic artery, portal vein, and bile ducts. Although lacking external landmarks, the portal lobes are further divided functionally into hepatic segments.
The four lobes of the liver are as follows:
- Right lobe. Positioned to the right of the inferior vena cava and gallbladder.
- Left lobe. Positioned to the left ligamentum teres.
- Quadrate lobe. Positioned posterior to the portal triad.
- Caudate lobe. Positioned anterior to the portal triad.
A. Visceral (inferior) view of the liver. B. Portal triad. C. Anterior view of the foregut with the body and pylorus of the stomach removed; the lesser omentum is also removed.
Functionally, the quadrate and caudate lobes are part of the left lobe because they are supplied by the left hepatic artery, drained by the left branch of the portal vein, and deliver bile via the left bile duct.
The left anatomical lobe, quadrate lobe, and a portion of the caudate lobe constitute the left portal lobe.


The liver receives a dual blood supply.
The hepatic artery supplies about 45% to 50% of the liver’s oxygen requirements, and the portal vein supplies the remaining 50% to 55%.
Hepatic arterial flow seems to be dependent on metabolic demand (autoregulation), whereas flow through the portal vein is dependent on blood flow to the gastrointestinal tract and the spleen.
A reciprocal, though somewhat limited, mechanism exists, such that a decrease in either hepatic arterial or portal venous flow results in a compensatory increase in the other.
The hepatic artery has α1-adrenergic vasoconstriction receptors as well as β2-adrenergic, dopaminergic (D1), and cholinergic vasodilator receptors.
The portal vein has only α1-adrenergic and dopaminergic (D1) receptors. Sympathetic activation results in vasoconstriction of the hepatic artery and mesenteric vessels, decreasing hepatic blood flow. β-Adrenergic stimulation vasodilates the hepatic artery; β-blockers reduce blood flow, and, therefore, decrease portal pressure.
+++++++++++++++
The liver receives a dual blood supply; approximately 30 percent of the blood entering the organ is from the hepatic artery, and 70 percent is from the portal vein. The proper hepatic artery is a branch of the common hepatic artery, one of the three major branches of the celiac artery. As it approaches the liver, it divides into right and left hepatic branches that enter the liver and divide into lobar, segmental, and smaller branches. Eventually, blood reaches the arterioles in the portal areas at the periphery of the hepatic lobules and, after providing oxygen and nutrients to the parenchyma, drains into the hepatic sinusoids. The majority of blood entering the liver is venous blood rich in nutrients and molecules absorbed by the gastrointestinal organs. Intrahepatic branches of the portal vein follow the arteries to the portal areas, where portal venules empty into the sinusoids from which molecules are extracted and added. Sinusoidal blood flows to the central vein of each lobule from which increasingly large veins are formed until typically three hepatic veins exit the liver to join the IVC.

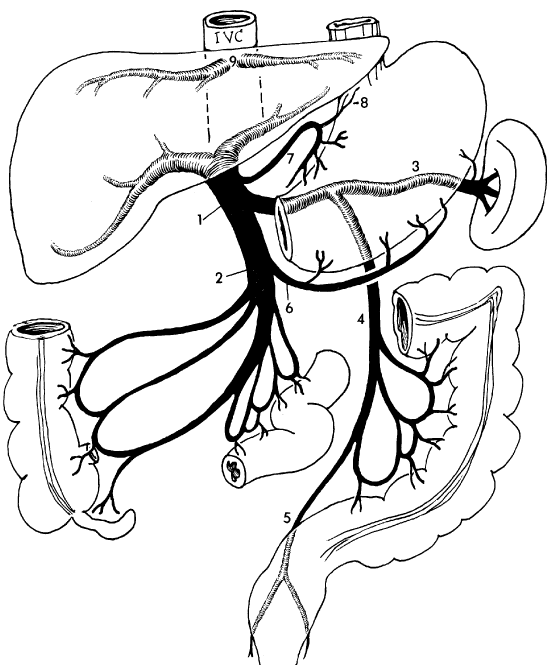
The portal system: 1 = portal vein, 2 = superior mesenteric vein, 3 = splenic vein, 4 = inferior mesenteric vein, 5 = superior rectal vein, 6 = right gastroepiploic vein, 7 = left gastric vein, 8 = esophageal vein, 9 = hepatic veins. (Reproduced, with permission, from the University of Texas Health Science Center Houston Medical School.)
The portal venous system arises from the capillary beds within the abdominal organs supplied by the celiac artery, superior mesenteric artery (SMA), and inferior mesenteric artery (IMA), and blood will flow to and through the liver for metabolism of its contained molecules. Veins from these organs for the most part accompany arteries of the same name. The portal vein itself is formed by the union of the splenic vein and SMV posterior to the neck of the pancreas. This short, wide vein ascends within the hepatoduodenal ligament, posterior to the bile duct and hepatic artery, and enters the liver through the porta hepatis. Typically, the IMV drains its blood into the splenic vein.
Portacaval (systemic) venous anastomoses occur at sites where blood may ultimately drain into the portal system and/or the vena caval system. If venous flow through the portal system is prevented by liver disease, for example, the absence of valves within the portal system veins allows reverse flow. This dilates the smaller veins, and blood is drained by veins emptying into the vena cavae. This occurs at several sites and may produce clinical signs or symptoms.
Sites of Portal-Caval Venous Anastomoses
| Portal Venous Drainage | Vena Cava Venous Drainage | Sign/Symptom | |
|---|---|---|---|
| Esophagus | Left gastric vein | Hemiazygous vein | Esophageal varices, bleeding |
| Rectum | Superior rectal vein | Inferior rectal vein | Hemorrhoids |
| Anterior abdominal wall | Paraumbilical vein | Intercostal vein | Caput medusa |
| Retroperitoneal | Duodenal, pancreatic, right and left colic veins | Lumbar vein | Intestinal bleeding |
+++++++++++++++++++++++++++++++++++++++
The celiac artery gives rise to the common hepatic artery.The common hepatic artery gives rise to the proper hepatic artery.
There are five branches of the hepatic artery: the right gastric, left gastric, gastroduodenal, left hepatic, middle hepatic, and the right hepatic. This group of arteries supplies blood to the pancreas, liver, gallbladder, stomach, and duodenal section within the small intestine.
[Need image}
The proper hepatic artery ascends in the free edge of the lesser omentum. As it approaches the liver it divides near the portal triad into the left and right hepatic arteries.
The common hepatic artery is a branch of the aorta off the celiac stem of the abdomen. There are five branches of the hepatic artery: the right gastric, left gastric, gastroduodenal, left hepatic, middle hepatic, and the right hepatic. This group of arteries supplies blood to the pancreas, liver, gallbladder, stomach, and duodenal section within the small intestine.
The right hepatic artery has a forked shape and supplies blood to the right region of the liver. Typically, the left and right hepatic arteries originate in a fork off the common hepatic artery and are positioned parallel to the portal vein and bile duct.
The right hepatic artery occasionally stems from the superior mesenteric artery. If this occurs, it is referred to as a replaced right hepatic artery. The replaced artery is travels through or behind the pancreatic head, near the main portal vein. In rare cases, it originates from the gastroduodenal artery.
Determining the position of the right hepatic artery is crucial for laparoscopic cholecystectomy, a type of surgery that uses very small incisions, a small camera, and special surgical tools to remove a person’s gallbladder.
The right hepatic artery gives rise to the cystic artery supplying the gallbladder. The right and left hepatic branches enter the liver and divide into lobar, segmental, and smaller branches.
The left hepatic artery supplies the left and quadrate lobes and a portion of the caudate lobe.
Eventually blood reaches the arterioles in the portal areas at the periphery of the hepatic lobules and, after providing oxygen and nutrients to the parenchyma, drain into the hepatic sinusoids. The majority of blood entering the liver is venous blood rich in nutrients and molecules absorbed by the gastrointestinal organs. Intrahepatic branches of the portal vein follow the arteries to the portal areas, where portal venules empty into the sinusoids from which molecules are extracted and added. Sinusoidal blood flows to the central vein of each lobule from which increasingly larger veins are formed until typically three hepatic veins exit the liver to join the IVC.

The portal system: 1 = portal vein, 2 = superior mesenteric vein, 3 = splenic vein, 4 = inferior mesenteric vein, 5 = superior rectal vein, 6 = right gastroepiploic vein, 7 = left gastric vein, 8 = esophageal vein, 9 = hepatic veins.
As it approaches the liver, it divides into right and left hepatic branches that enter the liver and divide into lobar, segmental, and smaller branches. Eventually blood reaches the arterioles in the portal areas at the periphery of the hepatic lobules and, after providing oxygen and nutrients to the parenchyma, drain into the hepatic sinusoids. The majority of blood entering the liver is venous blood rich in nutrients and molecules absorbed by the gastrointestinal organs. Intrahepatic branches of the portal vein follow the arteries to the portal areas, where portal venules empty into the sinusoids from which molecules are extracted and added. Sinusoidal blood flows to the central vein of each lobule from which increasingly larger veins are formed until typically three hepatic veins exit the liver to join the IVC (Figure 29-2).
The portal system: 1 = portal vein, 2 = superior mesenteric vein, 3 = splenic vein, 4 = inferior mesenteric vein, 5 = superior rectal vein, 6 = right gastroepiploic vein, 7 = left gastric vein, 8 = esophageal vein, 9 = hepatic veins. ( from the University of Texas Health Science Center Houston Medical School.)
The portal venous system arises from the capillary beds within the abdominal organs supplied by the celiac artery, superior mesenteric artery (SMA), and inferior mesenteric artery (IMA), and blood will flow to and through the liver for metabolism of its contained molecules. Veins from these organs for the most part accompany arteries of the same name. The portal vein itself is formed by the union of the splenic vein and SMV posterior to the neck of the pancreas. This short, wide vein ascends within the hepatoduodenal ligament, posterior to the bile duct and hepatic artery, and enters the liver through the porta hepatis. Typically, the IMV drains its blood into the splenic vein.
Portacaval (systemic) venous anastomoses occur at sites where blood may ultimately drain into the portal system and/or the vena caval system. If venous flow through the portal system is prevented by liver disease, for example, the absence of valves within the portal system veins allows reverse flow. This dilates the smaller veins, and blood is drained by veins emptying into the vena cavae. This occurs at several sites and may produce clinical signs or symptoms.
Sites of Portal-Caval Venous Anastomoses
| Portal Venous Drainage | Vena Cava Venous Drainage | Sign/Symptom | |
|---|---|---|---|
| Esophagus | Left gastric vein | Hemiazygous vein | Esophageal varices, bleeding |
| Rectum | Superior rectal vein | Inferior rectal vein | Hemorrhoids |
| Anterior abdominal wall | Paraumbilical vein | Intercostal vein | Caput medusa |
| Retroperitoneal | Duodenal, pancreatic, right and left colic veins | Lumbar vein | Intestinal bleeding |
-
Hemorrhage from the liver can be controlled by clamping the hepatoduodenal ligament (Pringle maneuver), which contains the hepatic artery and portal vein.
-
The portal vein drains blood from organs supplied by the celiac artery, superior mesenteric artery (SMA), and inferior mesenteric artery (IMA).
-
Esophageal varices with bleeding is the most clinically significant symptom of portal hypertension.
Study Question
If you ligated the right hepatic artery, the arterial supply to which of the following portions of the liver would remain intact?
The correct answer is E.
The left hepatic artery supplies the left and quadrate lobes and a portion of the caudate lobe.
The portal triad lies between the caudate and quadrate lobes. The portal triad consists of the portal vein, proper hepatic artery, and the common hepatic duct. The portal vein is deep to the hepatic artery and the common hepatic duct.
- Proper hepatic artery. Branches from the celiac trunk via the common hepatic artery. The hepatic artery supplies oxygenated blood to the liver. The cystic artery arises from the hepatic artery to supply the gallbladder.
- Portal vein. Formed through the union of the splenic and superior mesenteric veins, deep to the pancreas. The portal vein collects nutrient-rich venous blood from the small and large intestines, where it is transported to the hepatic sinusoids of the liver for filtration and detoxification. The hepatic sinusoids empty into the common central vein, which empties into the hepatic veins and ultimately drains into the inferior vena cava. The flow of blood from one capillary bed (intestinal capillaries) through a second capillary bed (liver sinusoids) before its return by systemic veins to the heart is defined as the hepatic portal system.
- Common hepatic duct. The union of the left and right hepatic ducts forms the common hepatic duct. The common hepatic duct transmits bile produced in the liver to the gallbladder for storage.
The gallbladder lies on the visceral surface of the liver, to the right of the quadrate lobe.
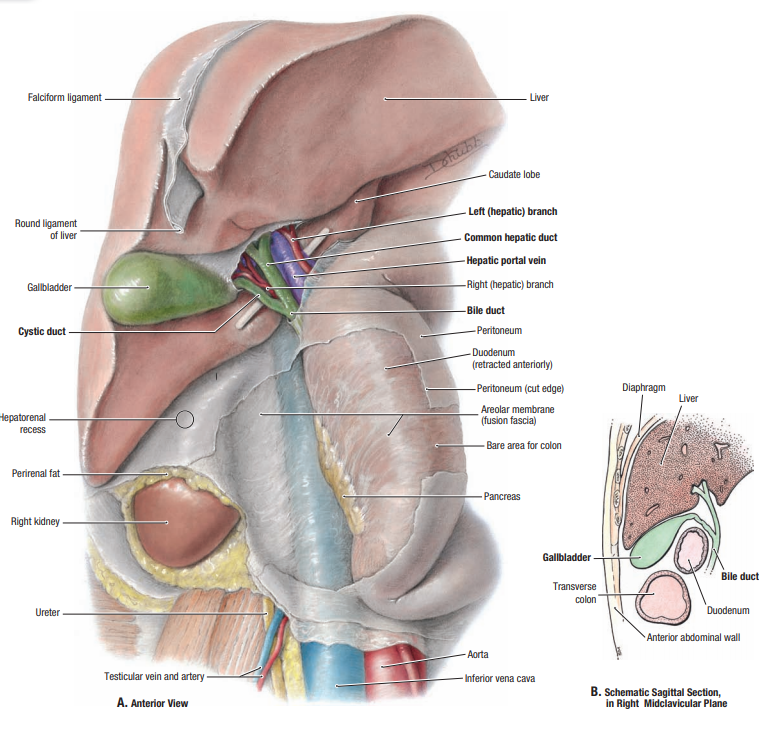
It stores and concentrates bile secreted by the liver.
Bile enters the cystic duct, which joins the common hepatic duct, becoming the common bile duct.
The common bile duct courses within the hepatoduodenal ligament of the lesser omentum, deep to the first part of the duodenum, where it joins the main pancreatic duct.
Together, the common bile duct and the main pancreatic duct enter the second part of the duodenum at the hepatopancreatic ampulla (of Vater).
The sphincter of Oddi surrounds the ampulla and controls the flow of bile and pancreatic digestive enzyme secretions into the duodenum.
If you ligated the right hepatic artery, the arterial supply to which of the following portions of the liver would remain intact?
Your patient who had cirrhosis has symptoms of esophageal varices. This is due to dilatation of the anastomosis between which of the following pairs of veins?
The correct answer is D. You answered A.
D. Esophageal veins drain to the left gastric and hemiazygous veins.